|
|
|
|
|
|
Welcome
Welcome to issue 05 of Recap, MICA’s regular communication on the College’s progress and planning around the return to campus for Spring 2021 and beyond.
Recap is also a place for dialogue, so we encourage you to use the Comment on This Topic button at the end of each story. We use your feedback to help build our shared understanding as One Team MICA.
And as always, some information may not apply to all programs and constituents, such as Open Studies. For specific information, please use the departmental directory at the end of this issue.
|
|
|
In This Issue: - Recap Revisit: Clarifying Operational Modes and Health Metrics
- Recap
AMA: You Asked Our Epidemiologists, They
Answered
- More Info: Upcoming End-of-Year Campus Closing and Furloughs
- What If: What If We Feel Sick?
- Transparency Report: Comments from Community
|
|
|
|
|
| RECAP REVISIT
Clarifying Operational Modes and Health Metrics
|
|
|
MICA introduced “Operational Modes” as a planning model for Spring Reopening in Recap 01 on October 13th. There was enough ambiguity in the initial description
that our community continues to have questions. We’re here with answers now.
As a reminder, the nature of Recap is to prioritize immediacy and transparency of information over absolute completeness and certainty—keeping everyone in the loop with our ongoing thinking and planning. Features such as Recap Revisit allows us to revisit topics as our thinking and planning evolve and mature.
What that said, let’s jump into clarifying Operational Modes.
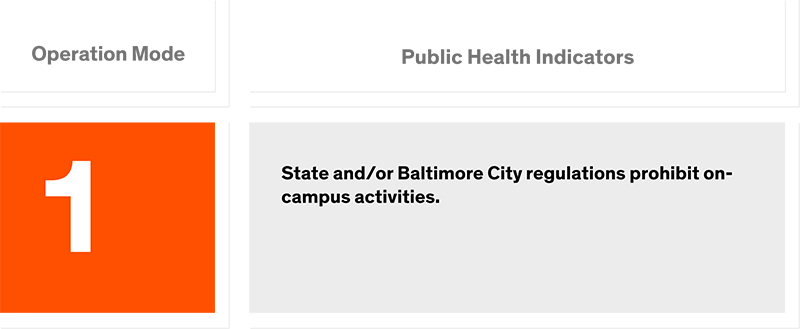
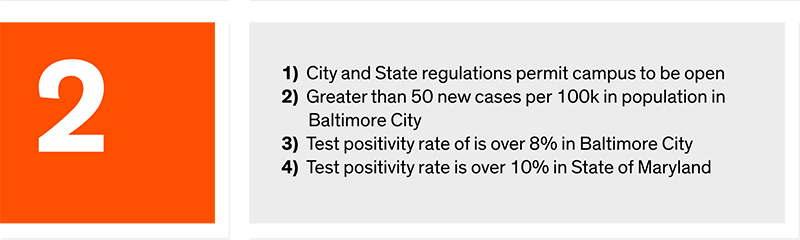
By the Numbers: What are we actually monitoring?
First, it’s important to note that when we launched the Spring Reopening Website and companion Operational Modes page, we included our best thinking at the
time for the public health metrics the College would be monitoring but did not include the specific values for those metrics. Given the unpredictability of the virus and our evolving understanding of it, it simply was too early to commit to that level of specificity.
Now with January right around the corner and MICA’s epidemiologists fully engaged, the College has finalized this information. The Spring Reopening website has been updated with it, but we are including the chart below for convenience.
|
|
|
|
|
|
|
|
|
|
|
|
|
To Trigger or not to Trigger: How does that actually work?
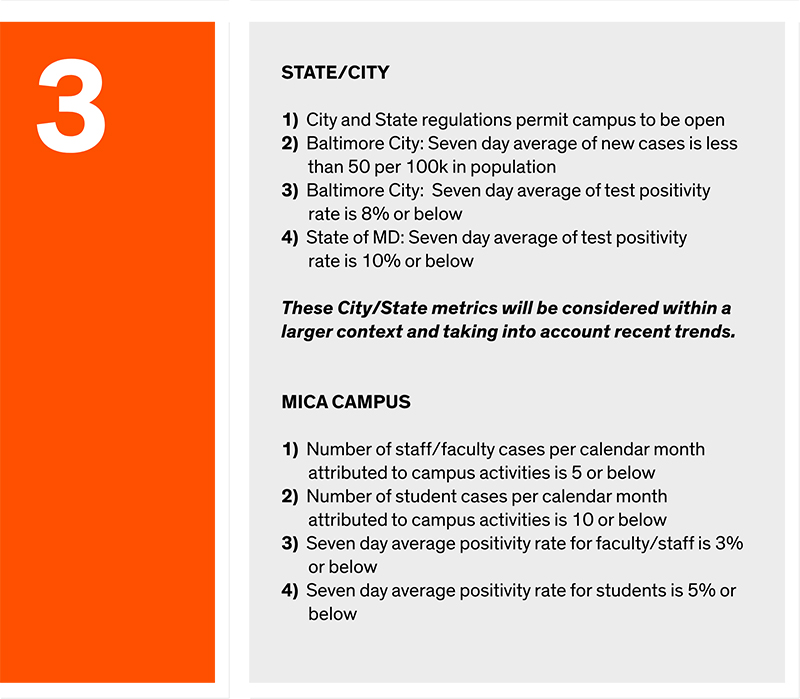
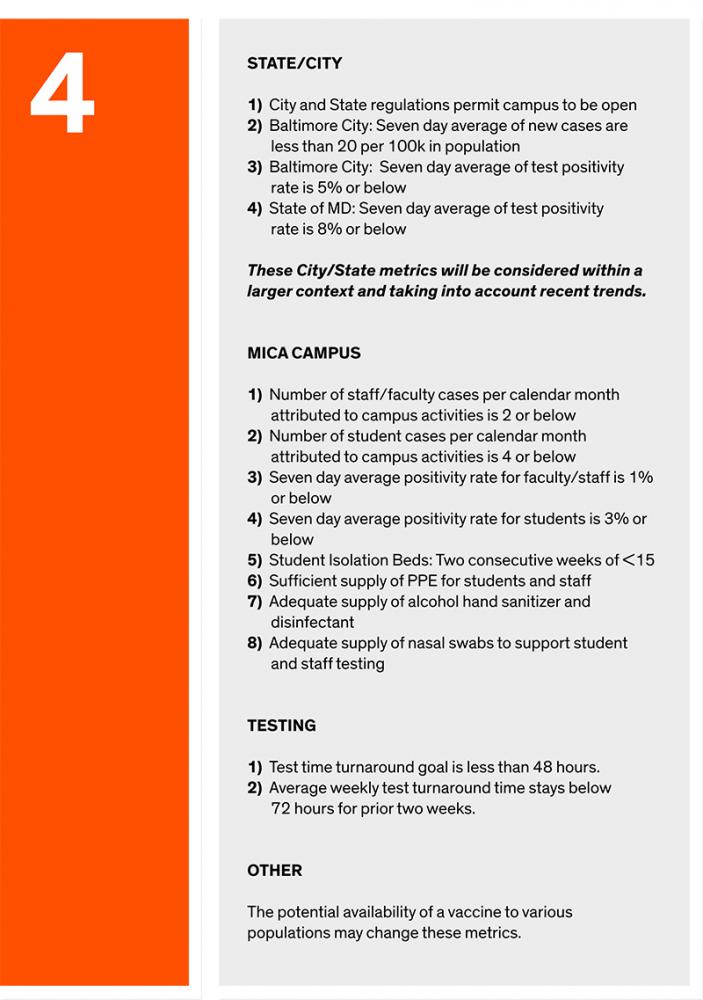
Many have reasonably assumed that the presence of clearly defined public health metrics and values assigned to each operational mode would mean that if those values are met, a change in Operational Mode will automatically be triggered. This is not the case. The metrics serve as guidance and information for further interpretation and decision making. In the words of MICA’s epidemiologists Dr. Anthony Harris and Dr. Jonathan Bagdhadi.
|
|
|
“None of these metrics can be used in isolation or without considering the broader context of the pandemic. The
metrics will be reviewed on a weekly basis by a group of key stakeholders and University of Maryland epidemiologists. These metrics provide a guideline rather than an automatic trigger. We have set thresholds for each metric to help identify when risk may be considered elevated, but the decision to change or keep an operational mode will be up to campus leadership.”
|
|
|
Ramp Up / Ramp Down: How Flexible is the On Campus Experience, Really?
Perhaps the area of most confusion was that of “ramping up and ramping down” the level of on-campus activity based on evolving public health conditions. Many were left with the impression that MICA could move from, say, OM3 to OM4 in the middle of the semester, suddenly filling on-campus classrooms with students and faculty. While this is a reasonable conclusion to reach, it’s definitely not the case. In fact, given the extraordinary level of effort and planning involved in moving curricula from in-person to remote and vice-versa, as well as the time and planning
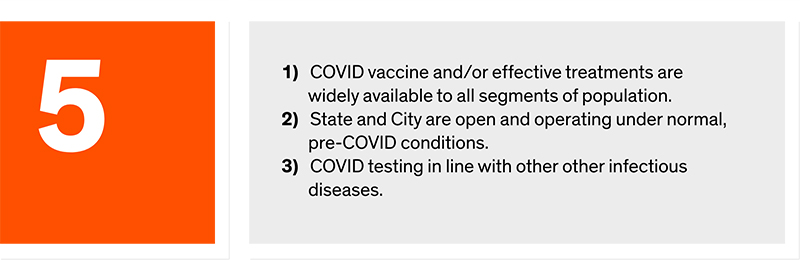
necessary to bring formal events like Art Walk back on campus, it will be logistically impossible for MICA to change Operational Modes upwards mid-semester. In short, Operational Modes are not intended to be an intra-semester framework, but rather one that will provide continuing structure for multiple semesters until MICA has returned to Operational Mode 5 — a fully open campus.
What can be adjusted based on the
public health metrics? To frame this, it’s best to consider the “ramping up and down” of on-campus activity will affect only the range of activity defined within an operational mode, and will not involve changing to a new, higher operational mode.
So to illustrate, Operational Mode 3 includes limited access to studios and shops, dining services, and co-curricular activities, and here are some examples of ways the on-campus experience within Operational Mode 3 might be adjusted:
If health conditions improve:
- Increase in-person engagements between faculty and students
- Enhancement of select academic support functions
- Open College Store for limited in-person shopping with physical distancing
- Increase cap on number of individuals allowed at in-person gatherings
- Expansion of in-person field and/or community based engagements
- Increase dining area occupancy
- Increase Fitness Center hours of operation
If health conditions decline:
- Increase frequency of testing to 2x per week
- Close down access to shops and fabrication spaces
- Eliminate in-person dining in Meyerhoff dining room
- Eliminate curbside pickup of equipment, books and College Store purchases
- Initiate a Stay at Home order for on-campus
- Suspend in-person field and/or community based engagements
- Suspend in-person co-curricular activities
- Resume telework for all non-essential staff/faculty
It is important to note that these are some potential ways that on-campus engagements could be adjusted based on health conditions and that none of these would be implemented without consultation with all MICA constituencies involved — faculty, staff, and students.
We hope this helps provide some additional understanding around Operational Modes, and, as always, please let us know if you have any additional questions about them by using the button:
|
|
|
|
|
|
|
| RECAP AMA
You Asked Our Epidemiologists, They Answered
|
|
|
The first Recap Ask Me Anything was introduced in issue 05. In that issue, we solicited questions from the community to be presented to MICA’s epidemiological experts, Dr. Anthony Harris, and Dr. Jonathan Baghdadi for their answers. Many of you responded with questions, and their answers are provided below.
|
|
|
|
|
Editors Note: We have received consistent feedback that Recap can be too long and too dense. We want to ensure everyone has the information they need for shared understanding, but recognize that lengthy emails may not be the best way to achieve this goal. We continue to look for new ways to efficiently communicate. To that end, Drs. Harris and Baghdadi’s responses are presented in a summarized (TL;DR) form here, with their full responses in an appendix at the end of this issue and in an FAQ found at mica.edu/art-articles/details/epidemiologist-ama-faq.
What is the efficacy of a PCR nasal swab test? What is the probability of a false negative or false positive? If the tests are to be self-administered, how do medical professionals ensure tests are performed correctly?
|
|
|
- PCR test are the most accurate we have
- Accuracy depends on whether or not
symptoms are present
- 90% accurate within 5 days of onset of symptoms.
- False negatives and positives occur but are rare
- PCR tests do not detect presence of virus during incubation period
- Nasal swabs for PCR tests do not
go deep into the nose
|
|
|
As MICA looks ahead to a partial reopening this Spring semester, what are the most important public health protocols you would advise the College and our community to be emphasizing?
|
|
|
- Masks should be worn in the presence of others but not needed when working alone in a private space
- Keep as much physical distance as possible when interacting with others
- Hand hygiene is essential especially when working in shared spaces
- Stay home and notify your supervisor if you are experiencing symptoms
- Eating in shared spaces is considered high risk and requires extra physical distancing.
- The protocols that MICA is developing will likely change over time, since the science behind COVID-19 is still evolving.
|
|
|
Thinking about the metrics that help inform MICA's Operational Modes, are they guidelines or hard and fast "triggers" where a change in one automatically alters MICA's Operational Mode?
|
|
|
- MICA will be monitoring a number of metrics both on campus and off
- None of these should be considered in isolation
- They are used as guidelines for review and interpretation
- They will not be used individually as “triggers”
|
|
|
Staying with the Operational Modes, and understanding that MICA is planning for a Spring opening in Operational Mode 3, what would you want to see to advise MICA to adjust down to Operational Mode 2 or up to Operational
Mode 4 for opening[HA4] ?
|
|
|
- TL;DR
- The Holiday season is expected to lead to a further increase in cases in the broad community
- We may recommend opening in OM2 if City and State metrics do not begin to trend downward in January
- We do not recommend opening in OM4 for Spring
- Moving to OM4 could be possible after the Spring
semester if there were very low positivity rates among students and employees throughout the Spring.
|
|
|
What is presently known about the efficacy of testing in general? What factors went into your recommendation to MICA that weekly, asymptomatic testing for individuals
regularly accessing campus was an appropriate approach?
|
|
|
- Recommendation for weekly testing is based on models that show it can expedite early detection.
- Weekly testing has become the practice for many colleges that have successfully reopened.
- More frequent testing can increase the duration of result reporting and risk supply shortages and is not recommended.
- If weekly testing does not strain available resources, increased testing frequency may be recommended in the
future.
|
|
|
You have recently
advised MICA that asking for a "pre-test" - a test taken several days to a week before travelling to campus - was not necessary. Can you walk us through that recommendation?
|
|
|
- Outside testing can be inconsistent with turnaround time and testing methodology leading to potentially unreliable results.
- Asking everyone to sort out their own testing could be chaotic and inequitable.
- Everyone returning to campus will instead be tested through MICA’s on-campus testing platform
- This ensures consistency and equity on a trusted platform.
- Individuals who can come to campus the week prior to classes starting for a test are encouraged to do so.
- Those who can not, should avoid in person contact until a negative test result is
confirmed.
|
|
|
What information can you share about the vaccines currently being developed and how they might become available to the general population?
|
|
|
- Up to 3 vaccines are on being considered for emergency authorization
- Healthcare workers, essential workers, and individuals at risk for severe infection are considered candidates for early vaccination
- The state of Maryland has not yet determined how to define essential workers, but faculty members may fall into this category.
- Vaccination will be voluntary
- Timing of vaccine distribution will depend on the supply that is provided to the state of Maryland
|
|
|
|
|
|
|
| MORE INFO
Upcoming End of Year Campus Closing and Furloughs
|
|
|
As you are aware, part of the College’s COVID-related budgetary measures is 10 days of mandatory leave without pay for all employees with
salaries over $50,000. To help facilitate this, the College will close the week between Christmas and New Years. This time is quickly approaching, so we’re providing a quick rundown with some important details.
|
|
|
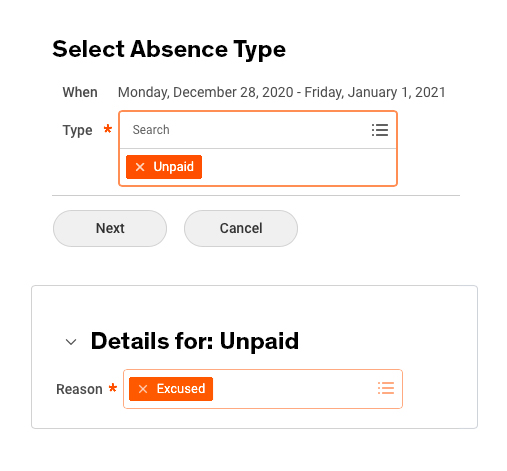
MICA will be officially closed Monday, Dec 28 through Friday, January 1.
You are encouraged, but not required, to use these five days of closure to fulfill part of the mandatory 10 days of unpaid leave.
If you choose to do so, you should register this unpaid leave within workday as “Unpaid/Excused” (see below)
|
|
|
|
|
In order to facilitate filing for unemployment and help exempt employees who need to take furlough time in full week increments, the traditional January 1 MICA holiday has transitioned to a floating holiday
that will need to be used by May 31.
You may choose to not use this time as unpaid leave and instead opt to use vacation time instead. However, you will still need to fulfill the 10 days of unpaid leave at a later date.
VPs will work with employees needing to perform emergency or essential college functions during this time to find alternative equitable
working arrangements.
You may apply for unemployment during these mandatory leave days.
You will not lose any MICA benefits during the unpaid leave period.
|
|
|
|
|
|
|
| WHAT IF
Real-World Questions from the Community
|
|
|
As a reminder, What if? Is an ongoing feature of Recap intended to help create a shared understanding of what the 2020 - 2021 academic year will look and feel like by posing real-world "what if" scenarios submitted by the community.
What if someone (staff, student or faculty) gets their temperature checked to get a wristband and their temperature is too high? Do they have to get tested before they are allowed back on campus? What if we are told to stay home for not feeling well. Do we have to take sick leave?
If a staff or faculty member is determined to have a temperature that is too high at one of the scanning stations on campus, they are to leave campus immediately and consult with their personal physician. They do not need to be tested for COVID before returning to campus but should check with their physician to determine if a COVID test is warranted. If someone is not feeling well and stays home, they need to take sick leave if they are unable to work from their home.
If a student is determined to have a temperature that is too high at one of the scanning stations on campus, they should immediately return to their place of residence and call the Student Health Center for appropriate guidance.
A new FAQ of on-campus COVID-19 protocols has been posted addressing this and other related questions. We’ll be covering this in the next issue of Recap, but you can check it here.
|
|
|
|
|
|
|
| TRANSPARENCY REPORT
Comments from the Community
|
|
|
|
|
|
|
|
|
| DEPARTMENTAL DIRECTORY
Please address specific questions to an appropriate departmental contact.
|
|
|
|
|
|
|
That’s it for this installment of Recap. Thank you for your engagement in this ongoing dialogue and building of shared understanding. If there are any topics you would like to have addressed in future installments, please provide your ideas here.
Stay safe and be well.
Coming Up in Issue 06: Staff Survey Results, On-Campus Protocols, and Furloughed Employee Communications
|
|
|
|
|
|
|
| APPENDIX
Recap AMA: Ask MICA’s Epidemiologists Anything
|
|
|
What is the efficacy of a PCR nasal swab test? What is the probability of a false negative or false positive? If the tests are to be self-administered, how do medical professionals ensure tests are performed correctly?
Full Response: The PCR test is considered the gold standard for diagnosis of COVID-19, and it is the test that we have the most experience with. However, it is not a perfect test. In particular, the performance of the PCR test varies depending whether someone with COVID-19 has symptoms and, if so, how long ago their symptoms began. If testing is performed around the time symptoms develop or within 5 days of onset of symptoms, the PCR test will detect >90 out of 100 individuals with COVID-19. Performance of the
PCR test is not as well understood in asymptomatic individuals, so it is hard to estimate the false negative rate, but based on comparisons between PCR and other types of tests, it should be the most sensitive test that is able to detect the most cases of COVID-19.
Unfortunately, false positives do occur, but they are relatively rare. In particular, we know that individuals who previously recovered from COVID-19 may continue to test positive by PCR, even though they no longer have active infection and they are no longer infectious to the people around them.
It is also important to remember that any kind of test may not detect SARS-CoV-2 while it is “incubating.” The incubation period is the time that passes between when an individual is exposed to the virus and when they develop infection. The typical incubation period for SARS-CoV-2 is 5 days. Thus, a negative test today does not guarantee a negative test
tomorrow. This is why testing is only one component of an effective campus policy.
The nasal swab specimen is easy to collect because it does not need to go far back into the nose. When researchers have compared the performance of PCR testing using self-collected specimens vs. specimens collected by trained professionals, the self-collected specimens are just as good. Many colleges have implemented testing protocols that require students and/or staff to self-collect specimens. These instructions may be helpful: https://www.cdc.gov/coronavirus/2019-ncov/downloads/community/COVID-19-anterior-self-swab-testing-center.pdf
As MICA looks ahead to a partial reopening this Spring semester, what are the most important public health protocols you would advise the College and our community to be emphasizing?
Full Response: At this point, important public health protocols are well-known.
Whenever possible, masks should be worn when in the presence of others. Eye protection, such as goggles or a face shield, can add an additional layer of protection. When
working alone in a private space, a mask is not needed.
When sharing a space with someone else, as much physical distance as possible should be maintained.
When using shared equipment, perform hand hygiene frequently and avoid touching your face.
If you have symptoms of a cold, such as fever, cough, sore throat, headache or muscle aches, notify your supervisor and do not come to campus. Loss of taste or smell is also a symptom that people with COVID-19 sometimes report.
On top of these basic steps, MICA has taken steps to enhance the environmental disinfection of campus spaces.
The most difficult thing to manage in terms of protecting your own health and the health of those around you will be eating and drinking. Eating and drinking are high risk activities because people like to do them together, and they cannot be done while wearing a mask. In our experience, the highest risk exposures almost always occur around a meal. If you would like to eat together with colleagues, try to find a big room and separate by as much space as possible. Indoor dining at bars and restaurants seems very risky, even if it is technically allowed by
city regulations.
Additionally, though they do not get as much attention, gyms are high risk. Forceful breathing can expel viral particles farther distances than normal breathing, and people may not feel comfortable exercising in a mask. Even a mask that is on at the begin of a workout may slide out of place or become soiled, which can reduce its protective effect[HA1] .
The protocols that MICA is developing will likely change over time, since the science behind COVID-19 is still evolving. We will work with them to stay up to date.[HA2]
Thinking about the metrics that help inform MICA's Operational Modes, are they guidelines or hard and fast "triggers" where a change in one automatically alters MICA's Operational Mode?
Full Response: MICA will be reviewing a number of metrics to monitor the level of risk to students, teachers, and staff. These metrics incorporate city data, state data, data from MICA on-campus testing, and data related to testing and isolation capacity. None of these metrics can be used in isolation or without considering the broader context of the pandemic. The metrics will be reviewed on a weekly basis
by a group of key stakeholders and University of Maryland epidemiologists. These metrics provide a guideline rather than an automatic trigger. We have set thresholds for each metric to help identify when risk may be considered elevated, but the decision to change or keep an operational mode will be up to campus leadership.
Baltimore City Dashboard:
Maryland State Dashboard:
Staying with the Operational Modes, and understanding that MICA is planning for a Spring opening in Operational Mode 3, what would you want to see to advise MICA to adjust down to Operational Mode 2 or up to Operational Mode 4 for opening[HA4] ?
Full Response: This is a tough question, because we anticipate that the number of cases of COVID-19 will likely increase after Christmas. If City or Statewide numbers stay very high and do not appear to be coming down in early January, we may advise campus leadership to move to reopen at Operational Mode 2. Similarly, if early on-campus testing reveals a high positivity rate among students or staff, we would advise shutting down some campus services. Our top priority is to protect staff, teachers, and students.
For the sake of caution, we would not recommend reopening at an Operational Mode above 3. In order to move to Operational Mode 4, we would hope to see very low positivity rates among students and staff during on-campus testing, reliable and consistent testing providing timely results, and high fidelity to recommendations for mask use. Though the decision is ultimately up to campus leadership, we would not recommend moving to Operational Mode 4 until one of the scheduled breaks in the semester.
What is presently known about the efficacy of testing in general? What factors went into your recommendation to MICA that weekly, asymptomatic testing for individuals regularly accessing campus was an appropriate approach?
Full Response: Much of what is known about different strategies for testing comes from epidemiologic models, which are based on the real world but are not the real world. We recommended weekly asymptomatic testing based on modeling that shows it can expedite early detection of COVID-19 infections and reduce the number of high-risk exposures to COVID-19. Weekly asymptomatic testing has become standard practices at many colleges that have successfully reopened.
We did not recommend more frequent testing based on what we
think will be feasible and safe in the long-term. Our goal is to maximize case detection while preserving capacity for testing, avoiding supply shortages, and preventing a backlog. The goal is not only that people get tested, but also that once testing is performed the results are available within a day or two.
If implementation of weekly testing is successful and does not strain available testing resources, we may recommend increasing the testing frequency.
We did not recommend more frequent testing based on what we think will be feasible and safe in the long-term. Our goal is to maximize case detection while preserving capacity for testing, avoiding supply shortages, and preventing a backlog. The goal is not only that people get tested, but also that once testing is performed the results are available within a day or two.
If implementation of weekly testing is successful and does not strain available testing resources, we may recommend increasing the testing frequency.
You have recently advised MICA that asking for a "pre-test" - a test taken several days to a week before travelling to campus - was not necessary. Can you walk us through that recommendation?
Full Response: The basic goal is that everyone coming back to campus will have a recent negative test. In our own experience, access to testing can be variable and the turnaround of results can be slow. In some cases, tests sent to commercial laboratories may take a week or longer to provide a result. In other cases, individuals who tried to access PCR testing were instead tested on a rapid platform, producing variable results. We were concerned that asking every individual to sort out their own plan for testing could lead
to chaos.
Instead, we have requested that all students, staff, and teachers returning to campus access testing through the MICA testing program. This way, testing can be accessed and resulted uniformly without confusion or delays with a testing platform that we trust. If possible, individuals who are local can arrange to come 2 or 3 days early to have their test performed, so that the results will be available by the time they arrive on campus. Teachers who cannot come early to be tested should avoid in-person instruction until after their first test has resulted negative.
What information can you share about the vaccines currently being developed and how they might become available to the general population?
Full Response: There are as many as three vaccines that may be approved via the emergency use authorization pathway by the end of this month. The manufacturers are Pfizer/BioNTech, Moderna, and Astrazeneca. The Pfizer and Moderna vaccines will be reviewed by the FDA on December 10 and 17, respectively. The date of review for the AstraZeneca vaccine has not been set yet. Each vaccine requires two shots, and
each has been demonstrated in phase III clinical trials to protect vaccinated individuals against infection in the weeks after they receive the second shot. Data on longer term immunity has yet to be released.
The CDC has released guidance regarding decisions about who should receive vaccination first. Healthcare workers, essential workers, and individuals at risk for severe infection are considered candidates for early vaccination. The state of Maryland has not yet determined how to define essential workers, but teachers will likely fall into this category. Vaccination will be strictly voluntary (but we will definitely get
it as soon as it is made available to me). Timing of vaccine distribution will depend on the supply that is provided to the state of Maryland and demand among potential candidates for early vaccination.
|
|
|
|
|